Why Is Leukemia Not Staged? Understanding Blood Cancer Assessment
It can be really confusing when someone talks about cancer, and then you hear that some cancers get a "stage" while others, like leukemia, don't. You might naturally wonder, you know, why is that? It's a common question, and honestly, it makes a lot of sense to ask why blood cancer seems to follow a different set of rules compared to, say, a solid tumor you might hear about.
Leukemia, as a matter of fact, is a cancer that starts in the blood-forming cells of the bone marrow. Unlike many other cancers that form a lump or a mass in one spot, leukemia cells are basically, well, they're already in your blood and bone marrow from the very beginning. This fundamental difference is really key to understanding how doctors approach it.
So, we're going to talk a bit about why the usual staging system, the one you hear about for breast cancer or lung cancer, just doesn't quite fit for leukemia. We'll explore how doctors actually figure out what's going on with leukemia, and how they decide on the best way to help someone who has it. It's a bit different, but it's all about getting the right picture.
- What Song Was Played At Jfks Funeral
- What Actress Just Revealed She Has Alzheimers
- Why Did Jfk Not Kiss The Popes Ring
Table of Contents
- The Unique Nature of Leukemia
- How Doctors Assess Leukemia Instead of Staging
- Different Types, Different Approaches
- Treatment Decisions: Beyond a Stage Number
- Why This Matters to You
- Frequently Asked Questions
The Unique Nature of Leukemia
What is Leukemia, Really?
Leukemia is a cancer of the blood. It begins in the soft, spongy center of your bones, the bone marrow, where blood cells are made. Normally, your bone marrow produces healthy red blood cells, white blood cells, and platelets. But with leukemia, something goes wrong, and the bone marrow starts making abnormal white blood cells. These cells, you know, don't work right and they tend to grow very quickly, crowding out the healthy cells.
These abnormal cells don't stay put, either. They travel through your bloodstream, which is, well, their natural environment. This means they can get to almost any part of your body. So, unlike a tumor that might start in one organ and then spread, leukemia is pretty much everywhere there's blood or bone marrow from the moment it begins. That's a really important distinction, actually.
Why Staging Doesn't Fit
When doctors talk about "staging" other cancers, they're usually talking about how big a tumor is and if it has spread from its original spot to other parts of the body. They use systems like TNM (Tumor, Node, Metastasis) to describe the size of the main tumor, whether it has spread to nearby lymph nodes, and if it has traveled to distant organs. This helps them understand how far along the cancer is and, in a way, sort of map its progress.
- Who Is The Boy Band Guy That Died
- How Old Was Bob Barker When He Filmed Happy Gilmore
- Whats Selena Gomezs Ring Worth
But with leukemia, because it's a cancer of the blood and bone marrow, it's already, by its very nature, systemic. It's not a localized lump that then decides to move. The abnormal cells are already circulating throughout the body. So, trying to "stage" it in the same way you would a solid tumor just doesn't make much sense, you know? There's no single "primary" tumor site to measure or track for spread, as it's already widespread.
This is why, as my text suggests, sometimes we ask "why" things are the way they are, and in this case, the answer lies in the very different way leukemia behaves compared to other cancers. It's a bit like asking why you don't use a hammer to drive a screw; it's just not the right tool for the job. The nature of the disease, you see, dictates how it's assessed.
How Doctors Assess Leukemia Instead of Staging
Instead of staging, doctors use a different set of tools and information to understand leukemia. They look at a variety of factors to classify the leukemia, determine how aggressive it is, and predict how it might respond to different treatments. This process is called "risk stratification," and it's basically how they build a picture of the disease's behavior.
Key Factors in Leukemia Assessment
When someone is diagnosed with leukemia, doctors gather a lot of information. This helps them figure out the best path forward. Here are some of the key things they look at:
- The specific type of leukemia: There are many different kinds of leukemia, and each one behaves a bit differently. Knowing the exact type is, you know, absolutely critical.
- Genetic and chromosomal changes: This is a really big one. Doctors examine the leukemia cells for specific changes in their genes or chromosomes. These changes can tell them a lot about how the leukemia might act and which treatments might work best. It's like finding a specific code within the cells, which is pretty amazing.
- Age of the person: A person's age can influence how they respond to treatment and how their body handles therapies. This is often a consideration, as older individuals might have different treatment tolerances.
- White blood cell count at diagnosis: A very high or very low white blood cell count can give clues about the disease's activity. This initial number, you see, provides a baseline for doctors.
- Whether it has spread to the central nervous system (CNS): Even though leukemia is in the blood, it can sometimes affect the brain and spinal cord. Checking for this is an important step, and it impacts treatment decisions.
These factors, and others, help doctors get a really detailed picture of the leukemia. It's much more nuanced than just a stage number, and it allows for a very personalized approach to care, which is, honestly, what you want when dealing with something like this.
Risk Stratification: A Different Kind of Roadmap
Instead of assigning a stage, doctors classify leukemia into different risk groups. This "risk stratification" helps them decide how aggressive the treatment needs to be. For instance, some genetic changes might put a person in a "low-risk" group, meaning their leukemia might respond well to standard treatments. Other changes might indicate a "high-risk" group, suggesting the need for more intensive therapy or perhaps a bone marrow transplant.
This process is, in a way, like creating a very specific roadmap for each individual's leukemia. It's not about how far it has spread, but rather about the particular characteristics of the leukemia cells themselves and how likely they are to respond to various treatments. So, it's a very tailored approach, you know, to treatment planning.
Different Types, Different Approaches
The world of leukemia is, well, quite varied. Knowing the specific type is absolutely vital because it guides everything from prognosis to treatment. It's not just one disease; it's a collection of related conditions, and each one, frankly, has its own unique quirks.
Acute vs. Chronic Leukemia
One of the first big distinctions doctors make is whether the leukemia is "acute" or "chronic." This refers to how quickly the disease develops and progresses. Acute leukemias, like Acute Myeloid Leukemia (AML) or Acute Lymphoblastic Leukemia (ALL), tend to progress very rapidly. They need immediate and often very intensive treatment because the abnormal cells multiply quickly and can cause serious problems in a short amount of time. It's a bit like a fast-moving storm, you know, requiring a quick response.
Chronic leukemias, such as Chronic Myeloid Leukemia (CML) or Chronic Lymphocytic Leukemia (CLL), typically progress much more slowly. People with chronic leukemia might not even need treatment right away; sometimes, doctors just watch and wait, a strategy called "active surveillance." The cells grow at a slower pace, which means there's more time to plan and, in some cases, less urgent need for intervention. This difference in speed is a really important factor in how doctors manage the disease, obviously.
Myeloid vs. Lymphoid Leukemia
Another major way to classify leukemia is by the type of blood cell that becomes cancerous. If the leukemia starts in myeloid cells (which normally develop into red blood cells, platelets, and some types of white blood cells), it's called myeloid leukemia. If it starts in lymphoid cells (which develop into lymphocytes, a type of white blood cell), it's called lymphoid leukemia.
This distinction is, you know, pretty fundamental. Myeloid and lymphoid cells are different at a basic biological level, and the cancers that arise from them behave differently and respond to different kinds of treatments. For instance, some targeted therapies work only for specific types of myeloid leukemia, while others are effective only for lymphoid types. So, getting this classification right is, well, absolutely essential for effective care.
Treatment Decisions: Beyond a Stage Number
Since leukemia isn't staged, treatment decisions are based on that detailed assessment we talked about. Doctors look at the specific type of leukemia, the genetic changes found in the cells, the person's age and overall health, and how the disease is affecting their body. This comprehensive picture guides the choice of therapy, which can include chemotherapy, targeted therapy, immunotherapy, or a stem cell transplant. It's a very individual process, honestly.
Personalized Plans
Because each person's leukemia is, in a way, unique, treatment plans are very much personalized. What works for one person with Acute Myeloid Leukemia might not be the best approach for another, even if they have the same general diagnosis. This is where those genetic tests and risk stratification really come into play. They help doctors pick the most effective treatments for that specific individual, which is, frankly, pretty incredible.
This personalized approach means that doctors are constantly evaluating the latest research and new therapies. It's a field that's always, you know, moving forward, with new discoveries helping to refine these treatment plans. So, it's not about fitting a person into a pre-defined stage; it's about building a treatment strategy that fits their unique situation, which is, arguably, a much better way to approach it.
For more information on how different cancers are classified, you might find it helpful to look at general cancer information from reputable sources, like the National Cancer Institute. Also, you can learn more about blood disorders on our site, and link to this page about leukemia treatment options.
Why This Matters to You
Understanding why leukemia isn't staged can really help clear up some confusion if you or someone you know is facing this diagnosis. It means that while the assessment process is different from what you might hear about for other cancers, it's just as thorough, if not more so. The focus is on the specific characteristics of the leukemia itself, which, in a way, makes the treatment very precise.
It's important to remember that not having a "stage" doesn't mean the cancer is less serious or that doctors don't know how to measure it. It simply means they use a different, more appropriate set of metrics for a disease that is, you know, fundamentally different. So, if you're ever wondering about this, just remember it's all about the nature of blood cancer.
Frequently Asked Questions
How is leukemia assessed if not staged?
Instead of staging, doctors assess leukemia by looking at the specific type of leukemia, the genetic and chromosomal changes in the cancer cells, the person's age and overall health, and the white blood cell count at diagnosis. They also check if the leukemia has affected the central nervous system. This information helps them classify the leukemia into different risk groups, which then guides treatment decisions. It's a very detailed process, you know, to get the full picture.
What are the different types of leukemia?
Leukemia is broadly classified into acute and chronic types, depending on how quickly the disease progresses. Acute leukemias (like ALL and AML) develop quickly, while chronic leukemias (like CLL and CML) progress more slowly. They are also classified by the type of cell involved: myeloid leukemia starts in myeloid cells, and lymphoid leukemia starts in lymphoid cells. So, you might hear about Acute Myeloid Leukemia (AML) or Chronic Lymphocytic Leukemia (CLL), for instance.
Does leukemia spread?
Leukemia is, by its very nature, a systemic cancer, meaning the abnormal cells are already in the blood and bone marrow from the start. So, it's not a matter of it "spreading" from one localized spot in the way a solid tumor might. The leukemia cells circulate throughout the body and can affect various organs, like the spleen, liver, and lymph nodes, and sometimes even the central nervous system. It's more about where the circulating cells decide to settle and cause issues, you know, rather than a spread from a primary site.
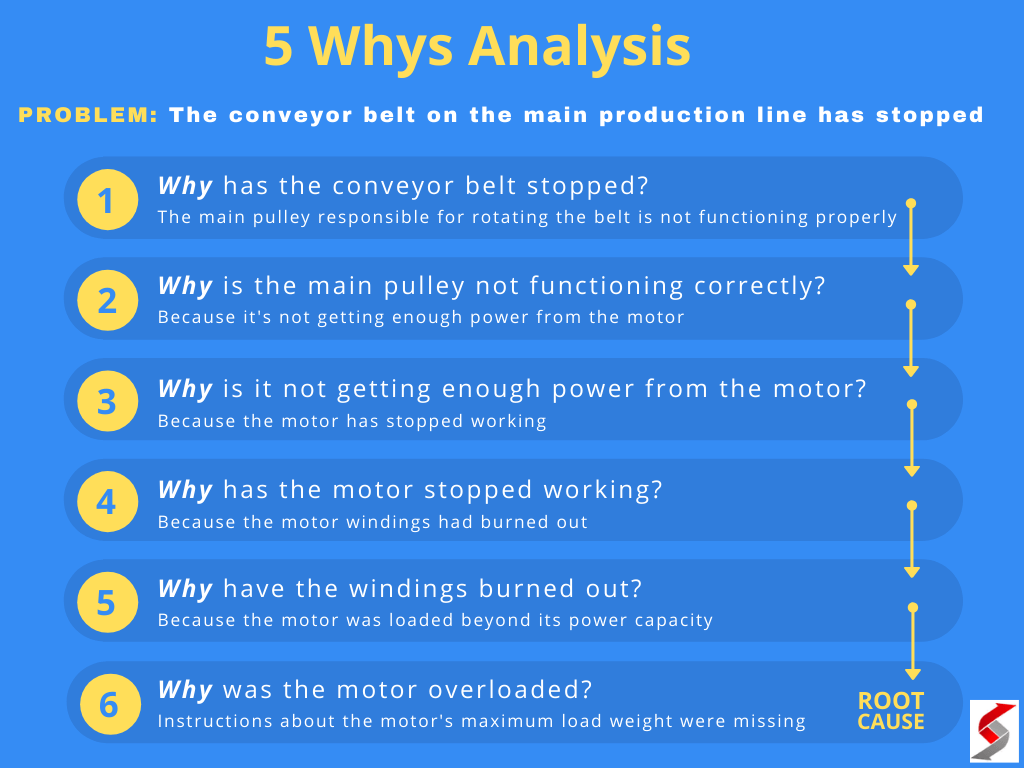
5 Whys Technique: Basics, Examples and Tips | The Business Analyst Job
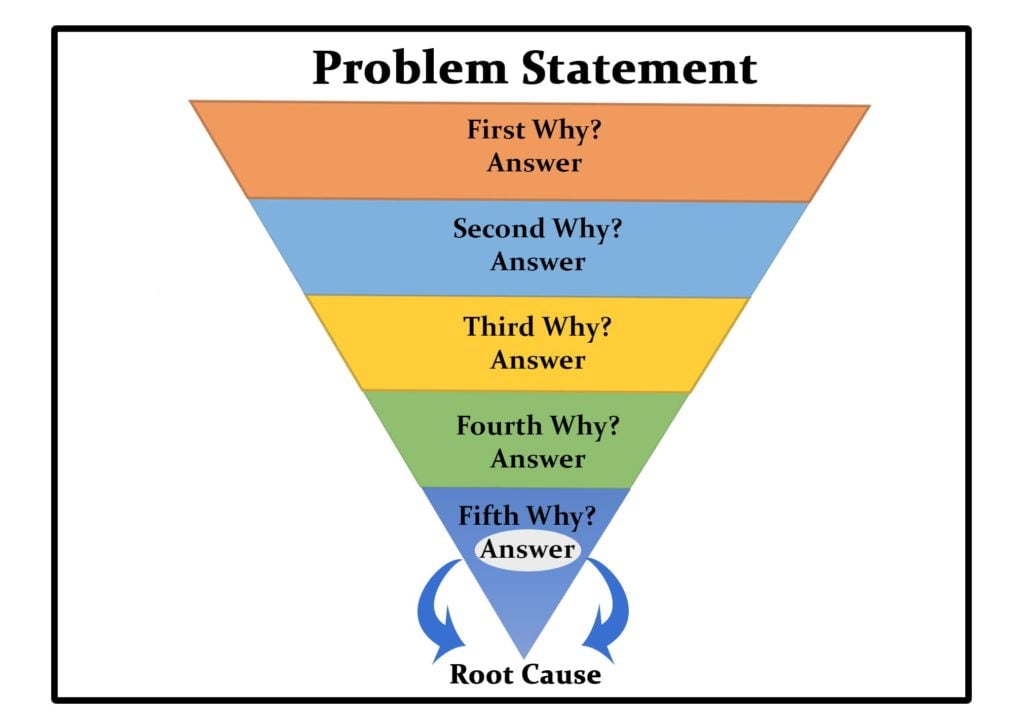
The 5 Whys Approach for Root-Cause Analysis: Definition, Example, and
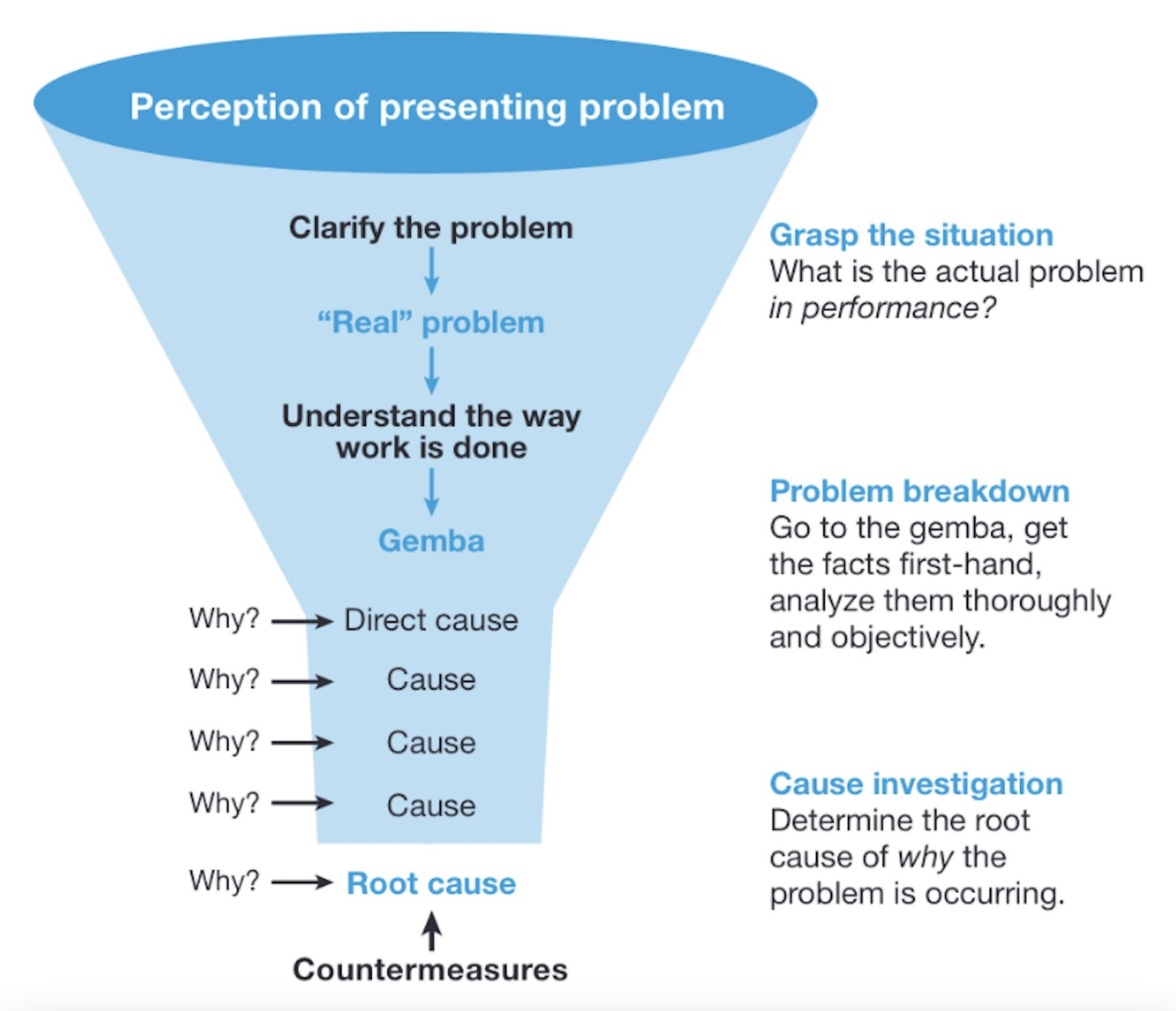
Five Whys Diagram Five Why's Anaysis
